


Implementation of an automated dispenser/injector in PET
Knowler, E.[1] Bartley, L.[1] Talboys, M.[1] Marshall, C.[1] de Wet, M.[1]
BNMS (British Nuclear Medicine Society) Spring 2018 – Birmingham (United Kingdom) – 14-16 April 2018
[1] Wales Research and Diagnostic Positron Emission Tomography Imaging Centre, Cardiff, CF14 4XN
Whole body fluorine-18 fluorodeoxyglucose Positron Emission Tomography/Computed Tomography (PET/CT) is one of the fundamental parts of staging in a number of oncology cases (Quinn et al, 2016). With PET/CT patient numbers rising there has been a significant increase in body and extremity doses to operators dispensing, administrating and scanning patients. A 2015 audit of staff doses in University Hospital of Wales PETIC highlighted the need for an automated dispenser and administration unit to achieve operator dose optimisation.

Fig.1. shows a graphic of the dose distribution ratio that staff receive for individual tasks associated with a PET scan, from dispensing to departure (red = most, green = least). The injection gives the radiographer the biggest dose and scanning gives the 2nd.
We monitor staff body and finger doses using a selection of devices. A ring thermoluminescence dosimeter (TLD) is worn on the middle finger of their dominant hand facing outwards to maintain consistency, then the readings are multiplied by a factor of 6.
As predicted, the audit from 2015 showed that the more dispenses a radiographer performed each month, the higher the TLD finger dose they received. Two radiographers were projected to receive doses higher than the annual dose constraint for non classified staff members (150mSv) (graph 1).
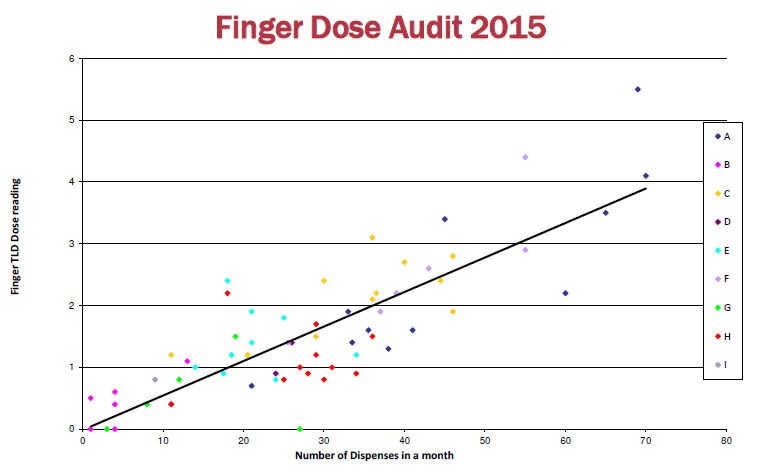
In light of this, the recommendations were to optimise procedures for dispensing and injecting, continually monitor possible contamination, increase the use of PPE when dispensing such as using tweezers and forceps, and ensure adequate training. In addition, radiographer A (graph 1) was asked to wear TLD sleeves over fingers to more accurately measure finger dose.
In response to the high finger doses to staff we made the decision to purchase an automatic injector.
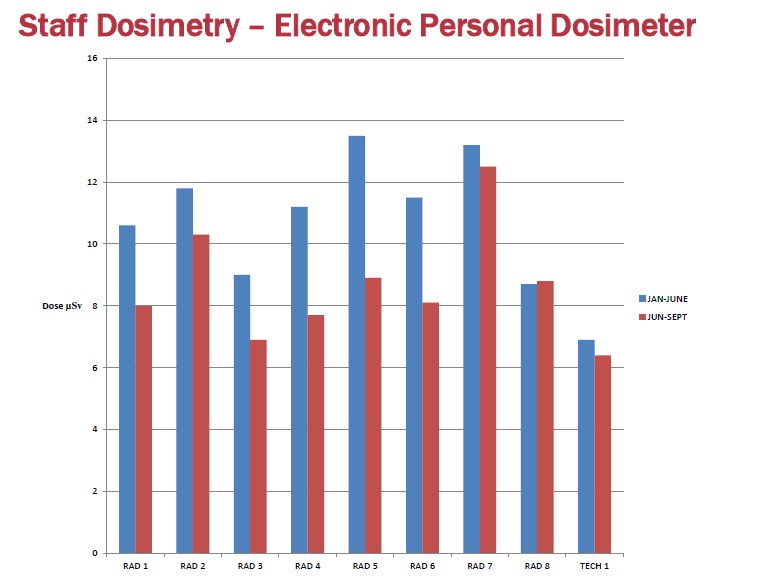
A detailed tendering process resulted in a Posijet V3 (Lemer Pax) being purchased and installed in early June 2017. Amongst the criteria were maximum vial volume, maximum radioactivity, minimum dispensing volume and footprint of the unit. As this is the first Posijet v3 system installed in the UK, an assessment was undertaken to determine the effectiveness of the unit to reduce operator doses. (graph 2)
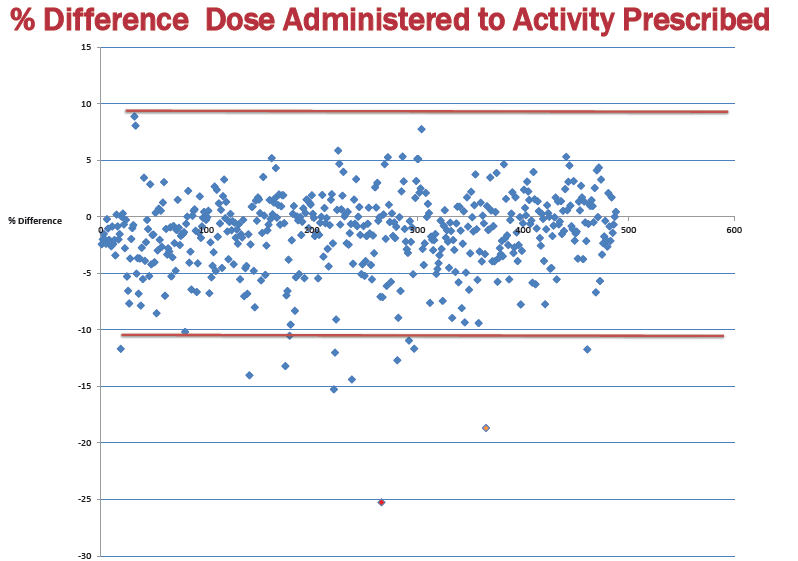
In the first 3 months post installation, we used the Posijet for 488 doses. We saw a 97.5% accuracy of dispensing within 10% of the diagnostic reference level (4 mBq/kg) against our 91% accuracy in 2016 with manual dispensing. Unfortunately the Posijet does not allow “topping-up” of the dose therefore we saw a range of 9% to -25% of activity administered against amount prescribed (graph 3).
The Posijet v3 is a reliable and functional system for the automated dispensing and administration of radiopharmaceuticals (FDG only at present). Staff are impressed by its ease of use and maneuverability despite its 380 kg weight. It has excellent traceability via use of a web application – data stored in spreadsheets for daily dispenses/administrations and quality control that can be downloaded.
Staff extremity and body doses fell during the first 3 months of operation demonstrating it’s success.
The issues noticed are:
- Inability to change the name of the operator after dispensing the dose.
- Unable to “top up” dispensed radioactivity when initial dose has decayed below 10% of prescribed dose.
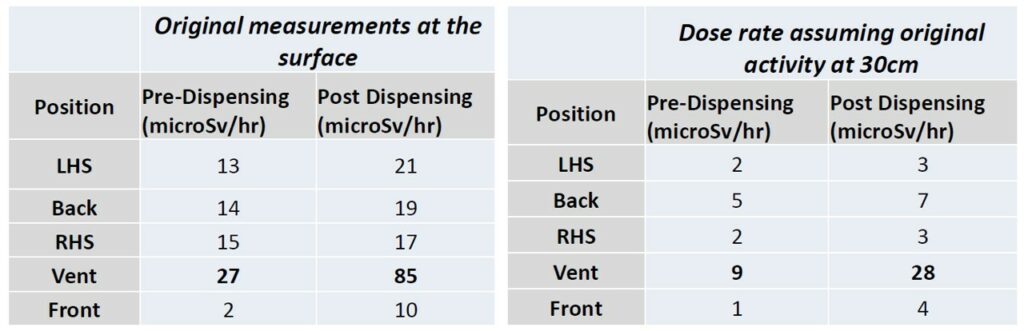
- Higher dose rate over ventilation aperture (fig 4).
- Staff made aware during training
- Prepare patient kits standing away from the vent
We are planning on performing an eye dose audit using a dedicated TLD to establish whether when loading the vial into the Posijet we receive a high eye dose, especially with the reduction within new legislation.
Peet, D. Morton, R. Hussein,M. Alsafi, K. and Spyrou, N. 2012. Radiation protection in fixed PET/CT facilities—design and operation. British Journal Radiology. 85(1013): 643–646.
Quinn, B. Dauer, Z. Pandit-Taskar, N. Schoder, H. Dauer, L. 2016. Radiation dosimetry of 18F-FDG PET/CT: incorporating exam-specific parameters in dose estimates. MBC Med Imaging. 16:41.
Click here for the digital version of the publication (in english)